

Abstract
Introduction:Continuous treatment with lenalidomide (len) is a new standard of care in frontline multiple myeloma (MM) (Facon. Blood. 2018;131:301-310; Pulte. Oncologist. 2018;23:734-739). The increased adoption of continuous len treatment and len maintenance highlights the need for active regimens for the treatment of MM that has relapsed or become refractory to len. Once-weekly carfilzomib (K) at 70 mg/m2 (Berenson. Blood. 2016;127:3360-3368; Moreau. Lancet Oncol. 2018;19:953-964) and twice-weekly K at 56 mg/m2 (Dimopoulos. Lancet Oncol. 2016;17:27-38) in combination with low-dose dexamethasone (d) have shown a favorable benefit-risk profile for the treatment of relapsed and/or refractory MM. This post-hoc analysis will assess the efficacy and safety of Kd in len exposed and refractory MM.
Methods: Individual patient data from the phase 1/2 CHAMPION-1 (CH-1), phase 3 ENDEAVOR, and phase 3 ARROW studies were pooled to evaluate progression-free survival (PFS), overall response rate (ORR), and safety for those with previous exposure or refractoriness to len treatment. The once-weekly Kd dosing schedule in CH-1 (Berenson. Blood. 2016;127:3360-3368) and ARROW (Moreau. Lancet Oncol. 2018;19:953-964) and the twice-weekly Kd dosing schedule in ENDEAVOR (Dimopoulos. Lancet Oncol. 2016;17:27-38) have been previously described. Patients who received once-weekly Kd at 70 mg/m2 in CH-1 and ARROW, and patients who received twice-weekly Kd at 56 mg/m2 from ENDEAVOR were included in the analysis. Patients were assigned to a group according to prior lines of therapy and previous len exposure: (1) combined CH-1 and ENDEAVOR patient population (N=39) that had received 1 prior line of therapy and was previously exposed but not refractory to len (Kd, 1 prior len exposed); (2) combined CH-1 and ENDEAVOR patient population (N=32) that had received 1 prior line of therapy and was refractory to len in the last line of therapy (Kd, 1 prior len refractory); (3) combined CH-1, ENDEAVOR, and ARROW patient population (N=65) that had received 2 to 3 prior lines of therapy and was exposed but not refractory to len (Kd, >1 prior len exposed); (4) combined CH-1, ENDEAVOR, and ARROW patient population (N=304) that had received 2 to 3 prior lines of therapy and was refractory to len in any line of previous therapy (Kd, >1 prior len refractory).
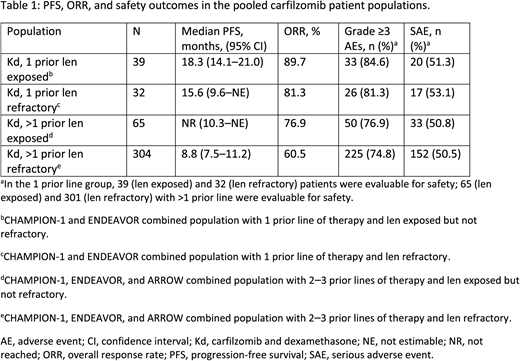
Results:PFS, ORR, and safety outcomes in the pooled len exposed and refractory patient populations are shown (Table 1). Len-exposed patients treated with Kd in first relapse had a median PFS of 18.3 months (95% confidence interval [CI] 14.1-21.0); PFS rate at 18 months was 54.0%. When len-refractory patients were treated with Kd in first relapse, median PFS was 15.6 months (95% CI 9.6-not estimable [NE]) and the PFS rate at 18 months was 43.1%. For len-exposed patients treated in second or third relapse, the median PFS for Kd was not reached (95% CI 10.3-NE) and PFS rate at 18 months was 57.1%. For len-refractory patients treated with Kd in second or third relapse, median PFS was 8.8 months (95% CI 7.5-11.2) and the PFS rate at 18 months was 27.8%. ORR was approximately 90% (Kd, 1 prior len exposed), 81% (Kd, 1 prior len refractory group), 77% (Kd, >1 prior len exposed), and 61% (Kd, >1 prior len refractory). Median K treatment duration (range) was 56.0 (4.0-213.0) months (Kd, 1 prior len exposed), 36.6 (1.0-201.1) months (Kd, 1 prior len refractory), 36.1 (1.1-210.7) months (Kd, >1 prior len exposed), and 34.0 (0.1-198.0) months (Kd, >1 prior len refractory). The incidence of treatment-emergent grade ≥3 adverse events (AEs) was 84.6% for patients in the Kd, 1 prior len-exposed group, 81.3% for patients in the Kd, 1 prior len-refractory group, 76.9% for patients in the Kd, >1 prior len-exposed group, and 74.8% for patients in the Kd, >1 prior len-refractory group. The rate of serious AEs in each of the pooled patient groups in this analysis is presented (Table 1).
Conclusion:The Kd doublet is effective and safe in MM patients relapsing on or after treatment with len, and for patients who are refractory to len. Although data are limited by small sample size, the median PFS of 15.6 months for Kd in len-refractory patients treated in first relapse is similar in magnitude to the median PFS reported for novel triplet therapy in this population.
Mateos:Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Berdeja:Genentech: Research Funding; Bluebird: Research Funding; Bristol-Myers Squibb: Research Funding; Takeda: Research Funding; Janssen: Research Funding; Amgen: Research Funding; Celgene: Research Funding; Glenmark: Research Funding; Novartis: Research Funding; Teva: Research Funding; Sanofi: Research Funding; Poseida Therapeutics, Inc.: Research Funding. Dimopoulos:Amgen: Honoraria; Bristol-Myers Squibb: Honoraria; Takeda: Honoraria; Celgene: Honoraria; Janssen: Honoraria. Siegel:Takeda: Consultancy, Honoraria, Speakers Bureau; Karyopharm: Consultancy, Honoraria; Merck: Consultancy, Honoraria, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Speakers Bureau; BMS: Consultancy, Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Speakers Bureau. Ho:Novartis: Honoraria; Janssen: Honoraria; Amgen: Honoraria; Takeda: Honoraria, Other: travel to meeting; Celgene: Other: travel to meeting. Huang:Amgen: Employment, Equity Ownership. Sersch:Amgen: Employment. Zahlten-Kumeli:Amgen: Employment, Equity Ownership. Kimball:Amgen: Employment, Equity Ownership; WindMIL Therapeutics: Equity Ownership. Weisel:Amgen, BMS, Celgene, Janssen, and Takeda: Honoraria; Amgen, BMS, Celgene, Janssen, Juno, Sanofi, and Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen, Celgene, Janssen, and Sanofi: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal